Thyroid biopsy - Ultrasound Guided Thyroid Fine Needle Aspiration Biopsy - FNA
An ultrasound-guided fine needle aspiration biopsy uses sound waves to help locate a nodule or abnormality within the thyroid and remove a tissue sample for examination under a microscope. The procedure is less invasive than surgical biopsy, leaves little to no scarring and does not involve exposure to ionizing radiation.
This procedure requires little to no special preparation.
Tell your doctor about any medications you're taking, such as aspirin or blood thinners.
What is Ultrasound-Guided Fine Needle Aspiration Biopsy of the Thyroid?
During a fine needle aspiration biopsy of the thyroid, a small sample of tissue is removed from the thyroid gland.
The thyroid gland is located in front of the neck just above the neckline and is shaped like a butterfly, with two lobes on either side of the neck connected by a narrow band of tissue.
Nodules or abnormalities in the body are often detected by imaging examinations. However, it is not always possible to tell from these imaging tests whether a noduleis benign (non-cancerous) or cancerous.
A needle biopsy, also called a needle aspiration, involves removing some cells—in a less invasive procedure involving a hollow needle—from a suspicious area within the body and examining them under a microscope to determine a diagnosis.
What are some common uses of the procedure?
Thyroid biopsy is used to find the cause of a nodule in the thyroid gland.
When a nodule is detected, imaging tests may be performed to help determine if it is benign (non-cancerous) or malignant (cancerous).
If imaging studies cannot clearly define the abnormality, a biopsy may be necessary.
How should I prepare?
Please notify your physician if you are taking any blood thinning agents, such as aspirin, Lovenox®, Plavix® or Coumadin®. Usually, no special preparations are required for this procedure.
What does the equipment look like?
The needle used is a thin, fine-gauge needle that is smaller in diameter than the needle used in most blood draws (usually a 25 or 27 gauge 1.5 inch needle). The aspiration may be done with a needle or with a needle that is attached to a syringe.
The syringe may be in a plastic or metal holder to make it easier for the doctor to aspirate the cells.
Ultrasound is used to guide accurate placement of the needle within the thyroid nodule.
Ultrasound scanners consist of a console containing a computer and electronics, a video display screen and a transducer that is used to do the scanning. The transducer is a small hand-held device that resembles a microphone, attached to the scanner by a cord.
Some exams may use different transducers (with different capabilities) during a single exam. The transducer sends out high-frequency sound waves (that the human ear cannot hear) into the body and then listens for the returning echoes from the tissues in the body.
The principles are similar to sonar used by boats and submarines.
The ultrasound image is immediately visible on a video display screen that looks like a computer or television monitor.
The image is created based on the amplitude (loudness), frequency (pitch) and time it takes for the ultrasound signal to return from the area within the patient that is being examined to the transducer (the device placed on the patient's skin to send and receive the returning sound waves), as well as the type of body structure and composition of body tissue through which the sound travels.
A small amount of gel is put on the skin to allow the sound waves to travel from the transducer to the examined area within the body and then back again. Ultrasound is an excellent modality for some areas of the body while other areas, especially air-filled lungs, are poorly suited for ultrasound.
How does the procedure work?
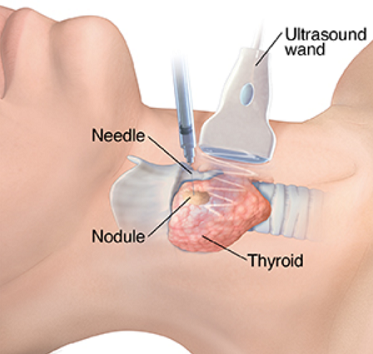
The physician inserts a fine gauge needle through the skin and advances it into the thyroid nodule.
Samples of the cells are then obtained and put on a slide for review by the pathologist.
How is the procedure performed?
Image-guided, minimally invasive procedures such as fine needle aspiration of the thyroid are most often performed by a specially trained radiologist with experience in needle aspiration and ultrasound.
Needle biopsies are usually done on an outpatient basis.
The neck will be cleansed with antiseptic. Medicine to numb the area may or may not be used.
An ultrasound transducer with a small amount of sterile water soluble gel will be placed on your neck over the thyroid nodule.
The radiologist will insert the needle through the skin under direct imaging guidance, advance it to the site of the thyroid nodule and aspirate samples of tissue.
After the sampling, the needle will be removed.
New needles will be reinserted if additional samples are required. Several specimens may be needed for a complete analysis.
Once the biopsy is complete, pressure will be applied to the area to decrease the risk of bleeding. A bandage may be placed if necessary.
No sutures are needed.
This procedure is usually completed in less than 30 minutes.
What will I experience during and after the procedure?
During the test, you will lie on your back with a pillow under your shoulders, your head tipped backward, and your neck extended.
This position makes it easier for the radiologist to access the thyroid gland.
You may feel some pressure on your neck from the ultrasound transducer and mild discomfort as the needle is moved to obtain the cells.
You will be asked to remain still and not to cough, talk, swallow or make a sound during the procedure.
Aftercare instructions vary, but generally you can resume normal activities and any bandage can be removed within a few hours.
The biopsy site may be sore and tender for one to two days. You may take nonprescription pain medicine, such as acetaminophen, to relieve any discomfort.
Who interprets the results and how do I get them?
A pathologist examines the removed specimen and makes a final diagnosis so that treatment planning can begin. Depending on the facility, the radiologist or your referring physician will discuss the results with you.
What are the benefits vs. risks?
Benefits
Risks
- The results of needle biopsy of the thyroid are close to 95% accurate for adequate biopsies.
- Needle biopsy is a reliable method of obtaining tissue samples that can help diagnose whether a nodule is benign (non-cancerous) or malignant.
- A needle biopsy is less invasive than open and closed surgical biopsies, both of which involve a larger incision in the skin and local or general anesthesia.
- Generally, the procedure is not painful and the results are as accurate as when a tissue sample is removed surgically.
- Recovery time is brief and patients can soon resume their usual activities.
- Bleeding at the site of biopsy.
- Infection.
- Injury to structures adjacent to the thyroid.
- Complications of thyroid biopsy are rare since the procedure is done under direct imaging guidance and with a fine needle.
What are the limitations of Needle Biopsy of the Thyroid?
In some cases, the specimens may be inadequate and the procedure may have to be repeated in order to obtain diagnostic results.